With Affordable Vaccines, Diagnostics and Medicines, Hepatitis Deaths Are Preventable
The Problem
Hepatitis kills approximately 1,400,000 people every year, more than HIV/AIDS. Every 22 seconds, someone dies of hepatitis; and globally, 4,100 lives are lost per day due to Hepatitis B (HBV) and Hepatitis C (HCV). With the availability of affordable vaccines, diagnostics and medicines, these deaths are entirely preventable.
CDAF’s Polaris Observatory has conducted Hepatitis disease burden analyses in over 100 countries/territories and has conducted economic impact analyses in 30 countries/territories. They all show that hepatitis elimination strategies are not only cost-effective, but cost-saving with a positive return on investment (ROI) within 25 years. Yet little action is being taken.
Except for a few countries/territories (Egypt, Mongolia, Pakistan and India), most programs in LMIC are small in scale, focused on special populations or they provide testing and treatment for free, making them neither sustainable nor scalable. The WHO 2030 elimination targets can only be achieved with programs targeting large populations and focusing on both HCV and HBV.
The majority of hepatitis burden is in LMIC (96% of HBV and 89% of all HCV infections). Most of these countries/territories lack the resources to fund the upfront investment needed to support an elimination program. And it is widely recognized that, unlike with HIV programs, large donors are not going to step forward with grants to fund hepatitis elimination programs.

“Financing the scale-up of testing is the key challenge to elimination.
Despite the burden of disease and existence of cost-effective interventions, there is currently no sign that a new global mechanism for funding viral hepatitis will be implemented to support the expansion of testing and treatment.
This places an onus on countries to develop new fiscal space to accelerate elimination, with may require innovative means of financing.”
Cooke G, Andrieux-Meyer I, Applegate T, et al., and the The Lancet Gastroenterology & Hepatology Commissioners. Accelerating the elimination of viral hepatitis: a Lancet Gastroenterology & Hepatology Commission. Lancet Gastroenterol Hepatol 2019; 4: 135–84
The Solution
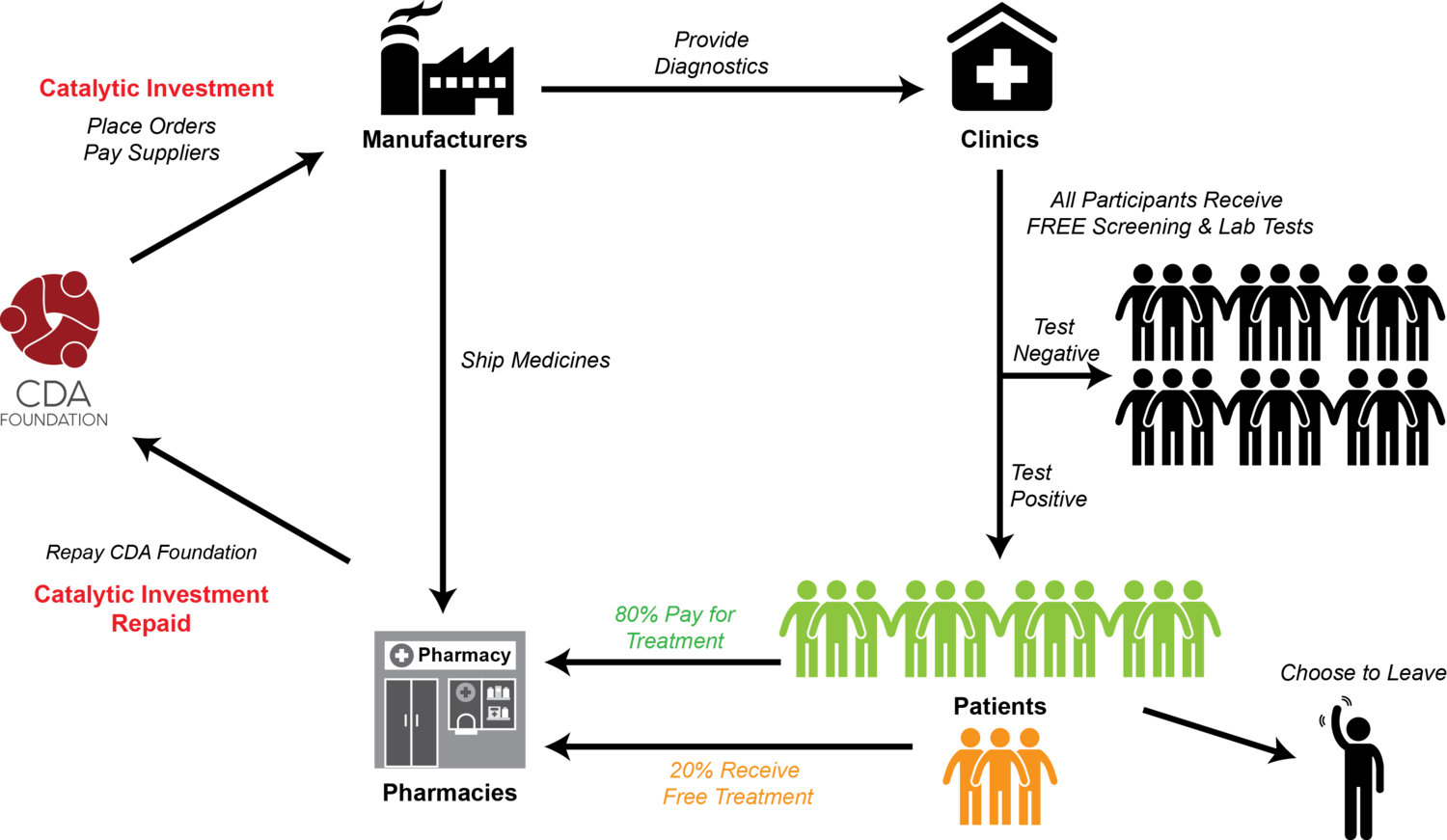
CDA Foundation has developed a scalable, sustainable catalytic funding mechanism that allows countries/territories to start their hepatitis elimination programs without a large upfront investment.
- The program relies on the premise that, even in LMIC, a majority of the population can afford to pay for treatment if drug prices and program costs are kept low.
- A modest markup on treatment pricing to those who can afford to pay can fund treatments for the smaller segment who cannot afford to pay. The mark-up can also fund all screening and laboratory tests.
- A small catalytic investment is needed to cover up-front costs/ working capital. Subsequent costs are paid for by the small markup on medicines, which also repays the initial catalytic investment.
- The program is based on a sustainable business model, not a donation-based model.
- Political-will is easier to achieve when governments are not required to support the full program with funding.
- National, rather than global focus opens investment opportunities to the broader community of local investors seeking local social impact.
- This approach represents a paradigm shift in funding global health programs.
Uzbekistan Hepatitis Elimination Pilot (UHEP) Program
To validate this concept at a large scale, CDAF has funded and is leading a pilot program in Tashkent, Uzbekistan in partnership with the Research Institute of Virology (RIV), the Uzbekistan Ministry of Health and a network of 13 Polyclinics serving the Tashkent region.
UHEP is NOT micro-elimination; it is a general population elimination program, which is essential to achieving WHO 2030 elimination targets.
Over a 12-month period, starting on December 6, 2019, UHEP will screen 250,000 people for HBV and HCV and provide treatment to an estimated 20,000 people. Approximately 1,000 people per day will be screened at community polyclinics. Most patients will be treated by general practitioners at the Polyclinics; patients with cirrhosis or other complications will be treated by liver specialists at the RIV.